Note: this post is not brief and ideally requires a bit of pre-reading:
In Ian Leslie’s longform article, “The Sugar Conspiracy,” we get a look into the history of nutrition, and the suggestion that politics and power dynamics play significant roles in the setting of dietary guidelines.
- The Sugar Conspiracy
- NutritionWonk's response discussing Ancel Keys' data
- If you're looking for a TL;DR version - see here.
In Ian Leslie’s longform article, “The Sugar Conspiracy,” we get a look into the history of nutrition, and the suggestion that politics and power dynamics play significant roles in the setting of dietary guidelines.
Leslie starts with a historical perspective, focusing on John Yudkin and his early hypotheses regarding sugar’s role in the aetiology of CVD. Yudkin’s studies, Leslie says,are cast down by the nutrition elite (i.e. Ancel Keys) at the time, in favor of recommendations that suggested limiting fat/saturated fat/cholesterol as the major drivers of CVD.
At face value, the story is one of redemption: Yudkin’s cast aside theories are now being realized by modern crusaders like Robert Lustig. In the article, Leslie states: “These sharp fluctuations in Yudkin’s stock have had little to do with the scientific method, and a lot to do with the unscientific way in which the field of nutrition has conducted itself over the years.” The narrative in this piece rests on this presumption. If Yudkin’s work was strong, but discarded by ivy tower academicians with easily bruised egos (I.e. Ancel Keys), we would indeed have a story of politics and the dietary guidelines. But what if Yudkin’s work wasn’t quite so rigorous?
As pointed out in NutritionWonk’s first post covering Keys' work, Yudkin’s initial 1957 Lancet paper posited a number of simple correlations of factors associated with CVD, without any real statistical analysis or consideration for covariates. Soon after this publication, Yudkin began writing about his hypotheses related to carbohydrates’ role in diet, and soon after, sugar’s role in cardiovascular disease. In addition to the plotted associations in his 1957 paper, his arguments rely primarily on observations of different ‘traditional populations’, his own case-control studies, and some human/animal experimental work done at the time.
Yudkins initial writings are reasonably mild; as in the 1957 Lancet paper, he notes that you can correlate a lot of things with CVD. In 1959, in JAMA, Yudkin, writing to clinicians, expresses that he finds the data linking animal fats to CVD ‘tenuous’ and believes that ‘the family physician should express the importance of physical activity and moderation in dietary habits. Especially he should advise the avoidance of overweight.’ Yudkin goes on to argue that the best way to do that is with a low carbohydrate diet, because it ‘not only controls weight easily but also limits fat intake’. Yudkin doesn’t cite his claim, but he begins to talk about carbohydrates more in future publications.
Yudkin Lancet, 1959
In his next Lancet paper, also from 1959, he begins to elaborate on his thoughts about calories, body weight regulation and the idea of the appestat (appetite-stat); something he believed was true because, now that food was less scarce after the wars, only 30 percent of the population was overweight, leaving most individuals able to maintain their body weight.
After discussing factors that might influence the appestat and food intake, he describes a couple studies done supporting his idea that carbohydrate isn’t as satiating as the other macronutrients; from his brief description of them, it’s not possible to tell whether or not they were randomized or appropriately controlled (though they don’t appear to be from his results).
One funny note: At the end of this article, he goes on to rant about the ‘anti-calorie’ folks and discusses the basics of thermodynamics.This is particularly ironic given that modern low-carbohydrate/insulin folks idolize him while rejecting what they see as the “conventional wisdom” about calories.
Yudkin Lancet, 1963
Yudkin’s work continues in a ‘63 paper in the Lancet, beginning by taking a very ‘Paleo’ approach where he lays out his theories about the change in man’s diet over time and its relationship to disease. When discussing myocardial infarctions, he notes that caloric imbalance and weight gain are major factors associated with their development, and proclaims that he believes highly palatable carbohydrate foods play a key role in the ‘failure to reduce caloric intake’.
One of his earliest claims, that carbohydrate foods, but not sugar specifically, are linked with CVD cites a review of lipoproteins and the effects of feeding by Albrink. This review presents two of the prevailing hypotheses at the time about the role of serum cholesterol and triglycerides in the aetiology of CVD, and the subsequent effects of carbohydrates, fat and total calories on these risk factors. Albrink notes that the discussion of lipids is not intended to imply causality, and hints that a low calorie/carbohydrate diet and high unsaturated fat diet might be best for controlling both.
Yudkin’s other proposal linking sugar to CVD in this publication cites one study (Cohen, 1963) of 20 Yemeni(te) families who recently moved to Israel (~5years) vs 20 families who had settled in Israel and lived there for some time (~20years). Families who had been settled for longer times had higher risks for chronic disease, including diabetes and heart disease. In order to compare new and old diets, recent settlers were asked to describe their diets back in Yemen, while settled families (~20 years in Israel) described their current diet. Other unpublished data from recently settled families in another survey were added as comparative groups, in addition to average European diets.
When comparing diets, the Cohen study notes that the recalled traditional diet relative to the settled diets contained significantly less sugar, but not total fat (~43g); additionally, higher vegetable fat consumption was common in the settled individuals. Very little information is given about the families besides diet; we’re not sure how the families were picked, their SES, etc.
In addition to differences in sugar, the difference in body weight between the settled and recently settled families was significantly different; males and females in the settled group were on average 8-9kg (~17-19lbs) heavier than their recently settled counterparts. Not unlike modern times, readers of this publication are left to ask: is it the sugar, or is it the calories?
However, this study was not entirely consistent with another publication (Toor 1960) at the time, which found that settled Yemenites consumed >60g of fat/day, and that those who had recently settled consumed only 30g per day. The recently settled families also reported consuming 800 fewer calories per day than their settled counterparts; comparing the data from Toor 1960 to Cohen 1963 also shows about an 800 kcal discrepancy between the caloric intake for recently settled immigrants.
Also not unlike modern times, we have significant disputes based on self-reported data. Whereas Cohen 1963 considered few other factors about the Yemenites besides dietary intake and weight, Toor 1960 performed substantial clinical evaluations and observed higher incidences of myocardial infarction among those settled in Yemen, correlating with their high blood pressure, blood cholesterol, and body weights/caloric intake.
While Cohen 1963 is an interesting paper, it’s unclear how generalizable those results are to the entire population of settled immigrants, and without any outcomes from these specific families, we’re left to make a lot of assumptions. Regarding the issue of body weight, there is significant debate about what the typical person from Yemen looked like.
Cohen claims that the diets of those living in Yemen were not semi-starvation or starvation diets based on their data from Yemenites living in Israel recalling their past diets, but this stands in opposition to claims from Nissan (Cohen cites personal communications with him), a doctor who spent 2 summers in Yemenites prior to immigration to Israel and claimed that these diets were (semi) starvation diets.
Following this personal communication citation, Cohen makes the claim that diets in Israel weren’t excessive - while not obese, it’s clear that Yemenites gained weight after spending time in Israel.
The issue of weight would be quite important to consider, as 1) it would predispose to diabetes, which was common in settled Yemenites and hypothesized at the time to predispose individuals to atherosclerosis, 2) Keys knew very well at the time that caloric intake/body weight affected cholesterol levels, limiting the impact of other dietary variables on total cholesterol (Keys 1953):

Ultimately, the data from different publications of families who immigrated to Israel from Yemen could be used to ‘support’ either Keys’ or Yudkin’s hypothesis; indeed, both Keys and Yudkin cite the Yemen immigrant studies to support their hypotheses, without noting the conflicting data. In both regards, the data are extremely weak. Neither study took into account the effects of smoking, noted to be common amongst Yemenites by Bruhn 1970, in his discussion of populations with low heart disease rates.

But, ecological data that’s unable to confirm or refute dietary hypotheses are not uncommon.
Bruhn 1970 concludes that the study of populations with low heart disease rates have generally failed to affirm or disprove most hypotheses, largely because most studies didn’t collect information on a number of risk factors outside of diet and blood cholesterol. And even in those that did include various risk factors did not examine populations long enough to determine variability (e.g. seasonal) in habits that might predispose to disease.
This is an important point to consider, because, in both Keys and Yudkin’s writing, you’ll notice that they go back and forth highlighting populations that don’t fit the others’ hypothesis (e.g. Keys points out that Cuba and Venezuela have high sugar intake and low saturated fat intake/CHD mortality; Yudkin, in his book Pure White and Deadly, cites other ecological data such as St Helena’s high sugar intake/low fat intake and high coronary disease rates).
Having come from a background in anthropology and having read about a number of traditional populations, I can certainly attest that the lack of thorough examinations and ambiguity in the existing data makes these ecological observations ideal for anyone trying to push a hypothesis, precisely because they are so limited in their ability to inform about the effects of individual dietary components without stronger population and trial data backing them. Consider: if everybody in a population gets hit by a car at age 45 and dies, saturated fat/sugar intake won’t correlate well with cardiovascular disease mortality!
Yudkin and Keys both cite observational/ecological data of sugar/fat intakes in different countries. In Yudkin’s 1963 Lancet article, and in multiple other publications, he uses his 1957 data to state the following:

This is something that Keys and Yudkin go back and forth on in the literature, claiming that their demonized macronutrient is associated with CVD best, even though intake of fat was associated with intake of sugar.
I cannot find any reference of Yudkin statistically analyzing these interactions(remember, he left us eye-balling the original associations) . Keys, however, was able to put forth data analyzing this interaction, supporting his hypothesis that saturated fat was more closely linked to CHD than sugar intake.
To clarify, while both Yudkin and Keys could throw out plenty of ecological data to support their respective hypotheses, only Keys actually analyzed effects of dietary components mathematically. Both are using observational data, but Keys (at this point) is staying more true to good epidemiological methods.
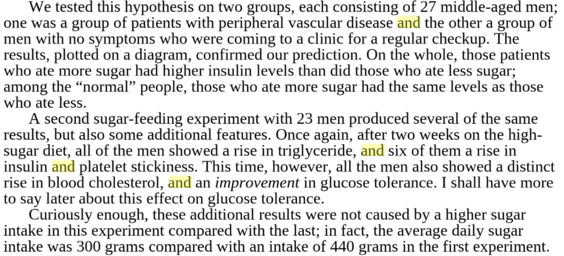
Moving out of the arena of ecological data, in 1964, Yudkin published again in the Lancet, this time utilizing a case control study design (another type of observational study). He was interested in describing the level of sugar consumed by patients with existing cardiovascular disease against ‘controls’. Yudkin used a questionnaire to assess sugar intake in individuals who had recently had a heart attack, those with peripheral artery disease, or controls, who had recently been hospitalized for an accident/healthy subjects in their homes.
Yudkin reportedly found nearly twice the intake of sugar in the CVD patient cases than his controls. Case-control study designs, as you might recall or notice on the evidence triangle, are of quite low quality. Today, they are primarily used to assess diseases that are rare because in common illnesses the odds ratios (which are used to approximate risk ratios in CC studies) are inflated.
{kind=link}
Beyond the issue of design, there were a number of limitations to this research. Yudkin was assessing intake in patients who already had a disease, much weaker than if he were to have prospectively assessed sugar intake (keep in mind Bradford-Hill criteria). The questionnaire used at the time had only been validated against food recalls, but not an objective measure of the actual amounts of sugar consumed (Yudkin, Roddy, 1966).
Further, the staff administering the sugar questions were not blinded to whether the individuals were a case or control, allowing for the potential that questioners were influenced by knowing that someone had CVD. Furthermore, while men were in the same age range, there was no effort to match based on other relevant characteristics that might affect metabolic health (eg body fatness) - a very crude case-control design.

Yudkin published a second paper in AJCN in 1967 with a similar design; this time however the questionnaire was modified so that patients could answer it on their own. Additionally, a non-hospitalized group of 20 men was included - these were the first 20 ‘age-matched’ individuals from a larger cohort of 247 factory workers. The same limitations from Yudkin’s first case-control study apply here with two exceptions; 1) there was no observer bias 2) this modified questionnaire had never been validated for determining sugar intake against dietary recalls.
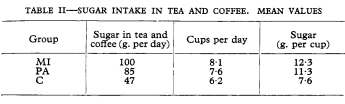
Assuming that we believe Yudkin’s questionnaire and the idea that patients were consuming 600 calories per day from sugar (in what looks like Starbucks Specialty Drinks meets the 1970s), it’s important to note that no group at the time was able to repeat Yudkin’s findings in other case-control studies.
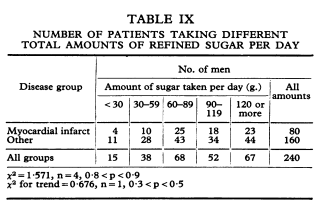
Of course, some of these studies were far from perfect themselves, some (Little, 1965, Papp, 1965) administering questionnaires months after hospitalization. However, other case-control studies were more rigorously done (Burns-Cox, 1969, Howell, 1969 ), taking into account factors beyond sugar intake, such as smoking, SES, and marital status and with much larger sample sizes. Howell used Yudkin’s own questionnaire and wasn’t able to reproduce his finding in over 1200 men (Yudkin’s n=70) .
Given the limitations of case-control design, it’s important to look at the literature to see what other stronger designs, like a prospective cohort study (assessing exposure before the disease), had told us about sugar; if there were no stronger designs out there, we might be able to say that Yudkin’s data was overlooked because it didn’t match others. However, one prospective cohort study was published at the time, which did not find a statistically significant effect of sugar intake with later CHD development (Paul, 1968), nor did it find intakes similar to Yudkin’s drastically high levels of sugar intake.
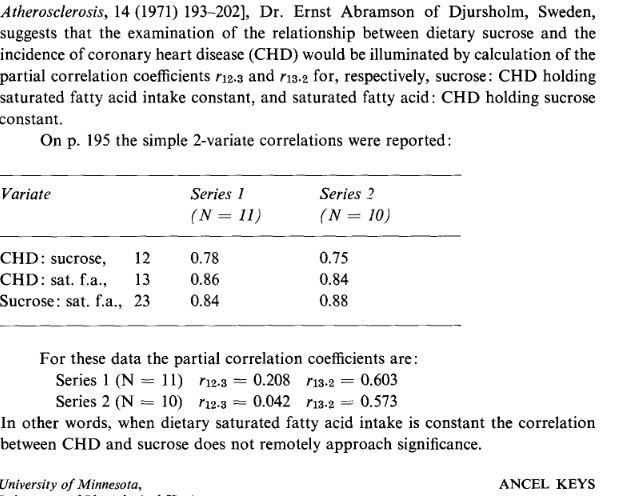
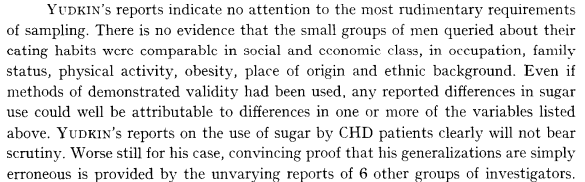
Yudkin’s failure to incorporate possible confounding factors in his case-control designs was an area of heavy critique at the time. The critiques were valid; apart from other unmeasured known risk factors that might affect CVD, data had emerged soon after suggesting that sugar intake was associated with smoking, a big risk factor for CVD (Paul, 1968, Bennett, 1970). Yudkin’s failure to account for confounding led to harsh words from Ancel Keys at the time (Keys, 1971):
Apart from his case-control data at the time, Yudkin attempted to put forth some experimental data to support his associations. One animal study cited by Yudkin relied on consuming largely sucrose based diets ( 67% by weight #yum) and didn’t account for relevant factors like changes in body weight (Cohen and Teitelbaum, 1964).
Another animal experiment was performed by Yudkin’s research group and compared a diet of 69% starch vs 69% sucrose to demonstrate alterations in body weight, liver fat and insulin sensitivity unique to source of carbohydrate. Again,Yudkin demonstrates few statistics and leaves us eye-balling the data ( Al-Nagdy, 1966).
It was noted at the time, however, that there were significant differences between man and animals, and between the different animal species themselves, calling into question their relevance in determining the harms of sucrose (Grande 1967). In chapter 16 of Yudkin’s Pure White and Deadly, he reviews the data on sugar’s effect on intermediate outcomes (e.g. cholesterol, triglycerides) in animal and human experiments, but rarely mentions the doses used in these studies; for example:

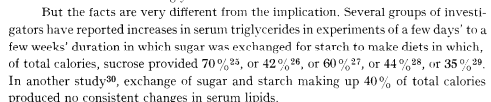
What Yudkin fails to note, and Grande 1967 points out, is that this dietary manipulation was the result of exchanging 500g of starch for 500g of sugar, equivalent to 73% of caloric intake! He does at one point mention levels from his own studies (Yudkin, 1969):
Not surprisingly, Keys critiqued these high levels of sugar in these experimental diets, questioning the relevance of large doses and small increases in triglycerides seen when acutely consuming very high sugar intakes (an argument still ongoing to this day!).

Keys was anything but subtle in his critiques of Yudkins work, but again, they aren’t invalid. Keys doesn’t appear to dismiss the issue of triglycerides though. He notes in his 1971 report that was directed at the issue of sucrose/CHD, triglycerides had yet to be shown to influence CHD independent of cholesterol in multivariate analyses from prospective studies (the first study was published in 1972).
Other figures at the time talking about sugar, namely Resier (mentioned in the Sugar Conspiracy as more of 'defender' of Yudkin), did address some of these criticisms but their arguments aren’t strong. Reiser argues that while it was true that the rise in triglycerides is transitory, there is the potential ‘danger that a defect or breakdown in this adaptation might produce triglyceridemia’, a speculative, claim with no cited evidence to support. He concludes this 1975 review, noting that sucrose hasn’t been shown to be an important risk factor in the etiology of heart disease in most of the population, but may play a role in specific subsets. He also speculates, based on data cited in this paper, that the type of fat consumed alongside the type of carbohydrate might be important, given that unsaturated fats blunted the rise in cholesterol seen in certain animal models fed high sucrose diets.

This publication summarizes much of the data that was available at the time the McGovern report/first dietary guidelines were set; you’ll note that both reports do advocate eating a low sugar diet, and a high complex carbohydrate diet at that, just not based on CVD outcomes (because, as noted above, sucrose hadn't been shown as a major risk fator for the majority of the population). A convenient fact left out by many of the ‘Dietary Guidelines Are Killing Us’ folk is that, regardless of the reason for not eating sugar, there have never been recommendations to eat high sugar diets.
Since much of “The Sugar Conspiracy” is about redeeming Yudkin’s hypotheses, I figured it relevant to note that he, more than once, made a case against trans-fats being involved in the pathogenesis of CVD.

What do we make of all of this?
Despite what Leslie’s ‘The Sugar Conspiracy’ would have you believe, there were significant limitations of Yudkin’s work and of the hypotheses surrounding sugar at the time. Leslie is quick to point out that Keys’ work was only based on correlations (and misrepresent aspects of the 7 Countries Study that NutritionWonk points out), but doesn’t discuss that Yudkin’s was based on weaker designs and experimental data with limited relevance. When you read through Keys’ work at the time, like his 1975 report on what was known about CHD, you’ll notice the large number of factors he considered and their relationship to CHD; he places a great emphasis on statistical modeling from prospective studies, and the need for future trials to test reducing the three major established risk factors at the time: serum cholesterol, smoking, and high blood pressure.
FWIW, I don’t think Yudkin was some terrible researcher; he clearly contributed meaningfully to the literature in a number of different areas and was an advocate for public health. In reading some of his book ‘Pure White and Deadly’, I found his chapter on ‘Can you prove it?’ quite entertaining, and thought that it gets at a lot of the issues nutrition has with setting recommendations and policy without strong randomized controlled trials; it actually reminded me a lot of the current debates on saturated fat and the multiple limited lines of evidence that have led to the recommendations (animal, epidemiological, biomarkers). Yudkin is quite forthright about admitting that his thoughts on sugar are just that: his thoughts/expert opinion with some evidence mixed in. He almost seems to me to not care much about the critiques of evidence quality; even in 1980 (well after Keys and others had critiqued the sugar work), he was still publishing non-randomized, uncontrolled sugar trials using doses of 260g of sugar (greater than 1000 calories/day) in acute settings (3 weeks). ¯\_(ツ)_/¯
What I find most interesting in reading all of this work is how much history repeats itself in nutrition: heavy focuses on observational studies, short term diet trials with arguably implausible consumption levels, and the need for longer randomized, controlled trials with outcome data to adequately test out theories. We’ve certainly come farther in experimental nutrition and epidemiological methods, but as far as really solidly answering the lingering questions about diet and long-term disease outcomes, we’ve not made as many massive leaps in settling debates that have been ongoing for 40+ years. Consider that we have no human randomized controlled trials showing that lowering sugar, or carbohydrates for that matter, affects cardiovascular events/mortality, a fact not put forth by the string of low-carbohydrate diet folks quoted by Leslie. Maybe that's the true 'Sugar Conspiracy'.
For those interested in the power narrative that this article paints, making it seem as though there are some nutrition elite bullying the little guys, consider a few points:
- The 1972 position statement from the American Health Foundation recommended replacing some sugar in the diet with starch.
- The 1957 American Heart Association position statement was quite cautious when talking about nutrition, calling out many fad diets and their ‘quackery’. When discussing fat, they noted that diet might play a role, but there were several criticisms of the theories surrounding the hypothesis. It was critical of diet histories and their accuracy, the link of fats to cholesterol but not outcomes, and the inability to disentangle high fat intake from low physical activity, high calorie intake, and other metabolic/dietary factors. “There is not enough evidence available to take a rigid stand on what the relationship is between nutrition, particularly the fat content of the diet, and atherosclerosis and heart disease.”
- The AHA 1961 statement, which included Ancel Keys, when discussing diet stated: “it must be emphasized that there is as yet no final proof that heart attacks or strokes will be prevented by such measures”.
- Similar to modern times, popular books also pushed the thesis, not just some ‘nutrition elite’. For example, John Gofman wrote a book entitled Dietary Prevention and Treatment of Heart disease.
- If you have access, I encourage you to read Karin Garrety’s ‘Science Policy and Controversy in the Cholesterol Arena’. She notes Keys’ advocacy in one line of the paper but tracks how diet and cholesterol recommendations came about across time. Her perspective is not exactly one of a ‘nutrition elite’ squashing dissenting voices to push their opinion. She notes the political pressures at the time from folks like President Johnson who wanted scientists to act on heart disease, even though there wasn’t new trial data to back the epidemiology data; she notes the public enthusiasm about low fat diets and the role the media played in disseminating the message; the difficulty in achieving a large enough sample size to show a reductions in CVD events matching that of the public enthusiasm; and the role of different industries in supporting and opposing new guidelines. It doesn’t, however, attempt to redeem past diet book writers by comparing their messages to current diet book writers.
History tells us that Keys' hypotheses 'won out', (though the DGAs have always recommended reducing sugar consumption). Whether that is because Keys was part of some ‘nutrition elite’ that bullied dissenting voices, or because his data had fewer limitations is open to some interpretation and a lot of anecdote. For me, Leslie’s authority argument falls apart substantially when considering the weak levels of data put forth by Yudkin. Maybe if Yudkin was a bit more charismatic, his hypothesis could have gone a bit farther, but the quality of his evidence likely wouldn't have taken him the distance.
"It follows that there must be some sort of mechanism in the normal individual which relates his food intake and caloric needs. Such a mechanism is called the Hyopothalamus which Joliffe has to graphically called the appestat" nowadays since the discovery of leptin & CCK and Grehlin we see more clearly how that mechanism works.
ReplyDeleteThis comment has been removed by a blog administrator.
ReplyDeleteAll the conservation of energy says is that there is SOME NUMBER we can calculate that does not cha ge after nature goes through its manifold changes. In fact, we already live in a universe where energy is NOT conserved. The expanding universe. CarbSane and Colpo are science illiterate CRANKS ��. ENERGY IS A CONCEPT AND ONLY CONSERVED LOCALLY, IN TIME TRANSLATI8NAL SYMMETRIC LAGRANGIANS. YES, I AM RAZWELL.
ReplyDeleteCALORIES HAVE N-O-T-H-I-N-G WHATSOEVER TO DO WITH THE CAUSAL MECHANISMS OF HOW HUMANS GAIN BODILY MATTER OF ANY SORT. CALIRIES ARE NOT ANYTHING THEMSELVES. MERELY AN ABSTRACTION.
To lose fat you must REMOVE, PHYSICALLY REMOVE AND EXCRETE ATOMS, CARBON ATOMS. ALL THOSE USED CARBON ATOMS ARE STILL THERE. STOP USING THEVTERM ENERGY FOR FUEL. HUGE PHYSICS MISTAKE, MORONS.
ReplyDeleteCALORIES HAVE NOTHING, NOTHING WHATSOEVER TO DO WITH LOSING MATTER FROM A BODY, YOU FOOLISH BLOGGERS......, ATOMS CANNOT BE BURNED OFF. TBE EXPRESSION "BURNING CALORIES" IS TOTAL NONSENSE AND MAKES NO SENSE SCIENTIFICALLY, NOR IS IT THE MECHANISM AT ALL OF HOW YOU LOSE FAT MATTER...... PACK OF IDIOTS ILLITERATE OF BASIC ATOMIC SCIENCE.