I've talked before about how there are a number of models within pharmacology/toxicology, that extend beyond just a linear dose-response relationship. One of the (arguably) more nuanced perspectives linking doses to outcomes is the hormetic dose response curve - that is, lower quantities of a compound exhibit greater bioactivity/effect than higher quantities of the same compound.

This goes against the way we typically think, where we imagine there is some linear/threshold model (we need a certain amount of a compound and more increases the effect until it plateaus or hits a ceiling). In a world where we have the ridiculousness of homeopathic dilutions, it's not always our first thought to consider that 'less' might be better.
For nutritional scientists, we generally work with 'U' shaped curves, where there is an intake that leads to deficiency, and an intake that leads to an excess. That is, low iron intake might lead to iron deficiency anemia, and high iron intake lead to gastrointestinal distress. Nutrition looks for that sweet spot in the middle where we fulfill human needs without getting to close to one end or the other.
As nutritional scientists have looked beyond just essential nutrients and at the rest of the food matrix, there's been no clear understanding of the dose-response relationship of non-essential bioactive compounds (NEBCs) found in many foods (mostly plant foods). Often, to see some positive effect, it takes very large dose, often drawing criticism from scientists - see this recent EJN study (1) that requires drinking gallons of red wine to reach the level of the compound studied. Many think that NEBCs (e.g. carotenoids, phenolics) have beneficial effects, particularly on processes like inflammation and cholesterol metabolism, though finding definitive evidence of this can be challenging. When these are isolated, they are often fed in large quantities, extending more into pharmacological doses rather than nutritional. The observed association between fruit and vegetable intakes (and general benefits of 'plant based' diets) and reduced incidence of chronic diseases has led some to be very enthusiastic about these compounds; however, the epidemiology is hardly rigorous - fruits and vegetables are often lumped together on questionnaires, and the amounts of NEBCs in foods vary significantly depending on a number of factors (eg post harvest time, soil they're grown in, exposure to pests, etc). Theories abound with quite limited evidence in this area - there is some to say that the compounds work within the context of the food matrix, and removing them disrupts important synergy; others suggest that the amounts of different compounds add to the total 'phytonutrient' load of the diet that is beneficial.
This question of dose plagues evidence-based nutritionists - how do you discuss something that occurs naturally in the food matrix, and will invariably be consumed, but dose isn't really worked out? Some is likely good, but how much do you need? How do you even know how much is in your food? While I find the field of research promising, I struggle with any public health message or clinical recommendations surrounding these components, especially in the day and age when Netflix documentaries push the magical anti-cancer properties of NEBCs (or just generally, 'antioxidants'). For any interested, a 2014 Advances in Nutrition paper (2) discusses some of the issues with setting recommendations for non-essential bioactive food components.
A new study (3) in Science Translational Medicine adds some information to this question of 'what the dose?!'. The study focuses in on one of the more popular resveratrol compound, found in grape skins and peanuts. The authors use labeled resveratrol to examine the pharmacokinetics of a 5mg and 1g doses. Not surprisingly, serum doses reach a higher concentration in the larger dose group, and significant inter-individual variation was found in the intestinal tissue of patients undergoing surgery that received the 2 doses. However, of interest to the authors, both the nutritional and pharmacological doses reached the intestines.

The authors follow up on this ADME data with a study in the Apc-min mouse model of intestinal tumorigenesis (a reasonable choice given that intestines might be a primary target for resveratrol). This model spontaneously generates intestinal adenomas, a phenotype that is worsened by the fat content of the diet (4). Using this model, with both a standard chow diet and a high fat diet, the authors fed two doses of resveratrol (0.00007 vs 0.0143%) and observed the number of intestinal adenomas. Interestingly, the authors observe opposite results depending on the dose of resveratrol and the type of diet.

When consuming the standard diet, the highest dose of resveratrol was most efficacious for reducing the numbers of adenomas per mouse. However, when consuming the high fat diet, the lower dose of resveratrol was most efficacious for adenoma number reduction.
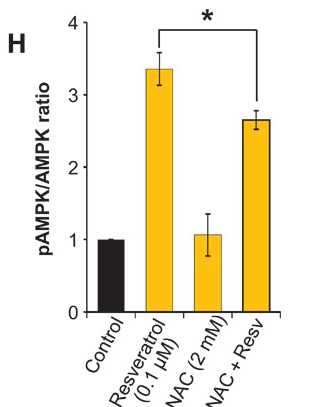
Mechanistically, the tissue and cell culture work suggest that AMPK phosphorylation is one of the targets of resveratrol in the intestine. However, no specific AMPK activator or inhibitor was used to show that this is completely responsible for the effects seen.
 |
| tissue |
 |
| cell culture |
 |
| One representative patient showing a non-linear relationship between pAMPK + resveratrol |
Many of these NEBCs are broadly called antioxidants and have been suggested to reduce oxidative stress, and DNA damage. However, this mode of action has been highly critiqued, as low levels of oxidative stress might be beneficial and certainly serve as potent intracellular signals. The authors observed an increase in ROS species within an hour of resveratrol treatment, and followed up with a co-culture experiment where cells cultured with resveratrol were also cultured with a potent antioxidant, n-acetylcysteine (NAC). One can see below that this blunted the effect of resveratrol, suggesting that resveratrol is not acting through an antioxidant effect but rather as a pro-oxidant.
While we can't assume that all chemicals act like resveratrol (indeed, a recent study on olive oil polyphenols suggest that more might be better (5)), nutritional doses of phytochemicals should certainly be considered in future research, as we attempt to define the optimal amounts of certain phytochemicals. Phytochemicals may just end up having a typical U-shaped curve like other nutrients, where some is good, too little is bad, and too much is bad/not as efficacious. Hopefully, this research will inspire other researchers to start quantifying the total dose of NEBCs necessary to achieve a desired physiological response, and we can start to address the 'more is better' paradigm. Likely, not all NEBCs will act in the same way.
As i've stated several times in the past (in the context of fatty acids), this individual nutrient approach is important (but should be complemented by whole food/diet approaches). As we enter a time when plant breeding and genetic engineering can create us crops with wide ranges of these compounds in our foods, it's necessary to consider the relative doses. Do we want high phytochemical foods in our food system? Until now, we've left it up to natural variation, but if we are to speak confidently, and in an evidence-based manner about these compounds, we need more studies like these.
1.http://www.ncbi.nlm.nih.gov/pubmed/24468941
2. http://advances.nutrition.org/content/5/6/693.full
3. http://stm.sciencemag.org/content/7/298/298ra117
4. http://www.pnas.org/content/94/7/3308.full
5. http://jn.nutrition.org/content/145/8/1692.full
1.http://www.ncbi.nlm.nih.gov/pubmed/24468941
2. http://advances.nutrition.org/content/5/6/693.full
3. http://stm.sciencemag.org/content/7/298/298ra117
4. http://www.pnas.org/content/94/7/3308.full
5. http://jn.nutrition.org/content/145/8/1692.full
Comments
Post a Comment